








National institutions must lead by example
regarding the publication of official documents

Click on the
octopus to return to
the top of the page
The original COMEX-based NORMAM-15/DPC saturation procedures,
which were adopted and published in Portuguese and English by the
Brazilian Navy Directorate of Ports and Coasts in June 2011, are an
evolution of the previously published COMEX MT-92 procedures that
are still in force in the French regulations.
They have been later on published and reinforced in 2019 in the CCO
Ltd Diving Management Study #5 “Implement Normam-15/DPC
saturation diving procedures” that rigorously conforms to this first
2011 edition, except that the gas values for the descent and the
storage periods that were missing in the official document have been
provided by Jean-Pierre Imbert, who worked as the COMEX company
diving manager at the time and who can be considered the lead author
of many COMEX procedures. The reasons for the reinforcements were
that several improvements to diving procedures have been adopted in
the industry since the creation and official publication of this table in
2011, necessitating the incorporation of these updates to keep this CCO
Ltd study current. Therefore, some complementary procedures from
the latest NORSOK standards U-100, the Diving Medical Advisory
Committee (DMAC), the International Marine Contractors Association
(IMCA), the UK Health and Safety Executive (HSE), and the French
Ministry of Labour are included in this study, along with conclusions
from relevant research such as the paper “A review of accelerated
decompression from heliox saturation in commercial diving
emergencies” by Jean-Pierre Imbert, Jean-Yves Massimelli, Ajit
Kulkarni, Lyubisa Matity, and Philip Bryson.
Incorporating these procedures into the original COMEX-based ones
results in a safe, cost-free alternative to recent saturation methods,
enabling operations at depths up to 350 m. This approach has been
favorably received by several scientists and companies, as it is cited in
multiple scientific studies and frequently downloaded. We can
therefore consider that, currently, the only more modern procedures
are those based on the sliding windows concept invented by Jean-
Pierre Imbert. However, these tables are available only privately and
are not freely accessible to the public.
It is also worth noting that two updates published by Brazilian
authorities were not considered, as these documents were only
available in Portuguese, and many in the scientific community, including
the lead author of these procedures, were unaware of them.
In 2023, the Brazilian authorities superseded the NORMAM-15/DPC
procedures with the NORMAM-222/DPC procedures, published both in
Portuguese and English. That has resulted in the need to compare
these new guidelines with those previously published in 2011 to
evaluate the evolution of these saturation diving procedures and,
consequently, determine whether they still conform to the original
COMEX procedure, whether additional reinforcements have been
introduced to comply with the latest safety practices, and whether
changes have been made that cause them to no longer conform to the
original decompression model.
Comparison method
A point-by-point comparison method was used to ensure no details
were missed. Thus, this involved writing the procedure steps into two
columns: one for Normam 15/DPC-2011 and one for Normam-
222/DPC. These steps were arranged side by side for easy
comparison, with chapters and sections separated by sufficient space
to avoid confusion.
As previously mentioned, Normam-222 saturation procedures were
compared only with those of the 2011 version of Normam-15, as the
"Study #5 CCO Ltd", published in 2019, is built on them and does not
incorporate the previously mentioned updates from the Brazilian
authorities. This comparison, available in the CCO Ltd Diving
Management Study #13, "Gap analysis between the Normam-15/DPC-
2011 and Normam-222/DPC Saturation Diving Procedures", showed
some differences, so we have contacted the Brazilian authorities for
clarification, and they have kindly responded. Their answers have been
introduced in the sections of this gap analysis that raised questions.
Results
The first point to note is that the English version should not be
considered valid, as essential elements such as the calculation method
for stabilization periods between the surface and 100 m have been
omitted. This omission results in the formula for exposures between
100 and 180 m being applied to both types of exposures, contrary to
the Portuguese version, which faithfully follows the original procedure
on this point. In addition, translations are not always precise. This
resulted in the use of the Portuguese version, which was translated
using the “DeepL” software, as well as the artificial intelligence
programs “Mistral” and “ChatGPT” when necessary. Nevertheless, for
convenience, the texts from the English version were used when they
were compliant. The cover of this English-translated version mentions
that it is not considered an original legal document. However, why
publish documents that are not verified to conform to the original? We
suppose there are sufficiently talented translators in Brazil who could
have done this work properly. To answer our remark regarding this
incorrect edition, the Brazilian authorities said that this item will be
adjusted in a future revision.
To conclude
Some may argue that what we propose is an unattainable ideal and
that maintaining the status quo is the only realistic option.
On the contrary, we believe that continuing along the current path risks
the collapse of the system initially designed to regulate and support
professional practices.
Such a collapse could lead to a world governed not by fairness and
merit, but by a handful of influential organizations competing to impose
their economic models, often relying on clientelism-based practices.
In such a world, professional organizations, companies, and individuals
would lose their rights and autonomy. Progress would depend not on
competence or innovation, but on securing the political favor of
dominant institutions. This scenario is the antithesis of the "democratic
world" so often promised by politicians.
To contribute to designing the "ideal diving world", we hold that the
principle of "every person to their trade", also known as "deference to
expertise", must be the rule. Therefore, states, supranational, and
international organizations must adopt transparent, science-based, and
consistent standard-setting practices. These practices should be open
to analysis, discussion, and, when necessary, criticism by professional
bodies and individuals.
To truly earn their legitimacy, national institutions must lead by
example. There is no other path forward.
Discussion
We must first emphasize that, as demonstrated in the CCO Ltd Diving
Management Study #5, it would have been possible to reinforce the
initial procedure, and thus avoid entering a process of validating a new
decompression procedure, by adding safety practices currently in use
in the diving industry without altering the key elements of the
decompression procedure, which include:
1.
The compression rate to the “storage depth”, stabilization stops,
and stabilization periods before diving, which are calculated to
manage phenomena such as compression arthralgia, narcosis,
and High Pressure Nervous Syndrome (HPNS).
2.
The maximum descent and ascent rates from and to the bell
3.
The maximum excursion distances and the excursion rules
associated with these distances.
4.
The published diving profile rules (for example, the “V” profile
NORSOK).
5.
The final decompression process.
6.
The recommended proportions of gas for each phase.
Regarding the previously mentioned lack of scientific documentation, it
must be remembered that, since antiquity, it has been common
practice for scientists to publish the conclusions of their work to the
scientific community before releasing them to the public. This practice,
which aims to ensure that the described study is scientifically
accurate, has also allowed us to refer to these works and use them
for further research. Scientists involved in creating diving
decompression procedures are accustomed to working this way. For
example, the latest explanations of the current evolution of the US Navy
tables are presented in the documents “Testing of Revised Unlimited
Duration Upward Excursions During Helium-Oxygen Saturations Dives”
published by Dr. Thalmann in 1990, “VVal-79 Maximum Permissible
Tissue Tension Table for Thalmann Algorithm Support of Air Diving”
published by Doctors Wane Gerth and David Doolette in 2012, and
“Manned Validation of a US Navy Diving Manual, Revision 7, VVal-79
Schedule for Short Bottom Time, Deep Air Decompression Diving”
published by Doctors Brian Andrew and David Doolette in 2020. The
studies that resulted in the creation of the Normam-15/DPC-2021 are
described in a document titled “Deep diving: The Comex experience”,
which has been written and published by Jean Pierre Imbert at the
Bergen conference in September 2005. More recently, Dr. Risberg, the
lead author of the editorial team of the Norwegian diving and
decompression tables (NDDT), has published a document entitled
"NDDT—Probability of Decompression Sickness", which details the
conceptual process undertaken by the team to create these
decompression tables.
Some may argue that the gas values mentioned in the Normam-
222/DPC have been in force in Brazilian waters since 2016 and that no
decompression incidents have been publicly reported, so this modified
procedure can be considered safe. However, this argument is
fallacious for the following reasons:
•
First, there is no data to verify this point accurately, considering that
many events may have gone unreported by companies and the
divers experiencing them.
•
Second, even if no visible decompression sickness incidents have
been reported, it does not mean that divers have not suffered from
undetected decompression sickness or various stresses related to
decompression that could lead to medical complications later. For
example, in a document titled "Saturation Diving: Physiology and
Pathophysiology," Alf O. Brubakk, John A.S. Ross, and Stephen R.
Thom state that while testing the US Navy's "Unlimited Excursion"
tables from 300 to 250 meters of seawater (msw), results showed
that all divers had significant amounts of vascular gas bubbles in
the carotid artery, the blood vessel supplying the brain. However,
none of the divers exhibited acute clinical symptoms. This
phenomenon was confirmed during upward excursions from 300
to 250 msw in an experimental saturation dive, where Dr. Brubakk
et al. found arterial bubbles in the carotid arteries of all six
participants, without resulting in clinical cases of neurological
decompression sickness. However, post-dive examinations revealed
a minor cerebral lesion in the diver with the highest number of
carotid bubbles. Therefore, we can consider that the naked eye and
feeling are not sufficient to detect some accidents and that only
tools such as doppler, echocardiography, bioimpedance, urine
testing, salivary testing, blood testing, magnetic resonance imaging
(MRI), etc., allow specialists to detect the effects of such not visually
detectable decompression accidents. The recent studies
“Commercial Divers’ Subjective Evaluation of Saturation”, “Vascular
Function Recovery Following Saturation Diving”, and “Hydration Status
during Commercial Saturation Diving Measured by Bioimpedance
and Urine Specific Gravity”, available in our database, are examples
of the use of such tools to identify the various stresses and not
visible decompression problems in relation to saturation diving.
To the best of our knowledge, there has not been any study based
on such research protocols that concludes that changing the initial
PPO2 of a COMEX-based saturation procedure to US Navy PPO2
values does not affect divers.
Based on the above and the elements mentioned in the previous
section, it is evident to us that the Brazilian authorities made several
undocumented and inconsistent modifications to key points, resulting
in the creation of a new decompression procedure with some critical
parts lacking scientific evidence.
In addition to the problem above, which results in the procedures
Normam-222/DPC no longer being compliant with the original ones
published in 2011, we must consider that numerous elements are
missing for an extended period of time, which demonstrates issues
regarding document control procedures and an obvious lack of
reactivity to address them. Consequently, we have considered that
these procedures cannot be viewed as relevant for the operations for
which they were created, and that the only procedures to be
implemented remain the NORMAM-15/DPC-2011, faithfully described
in the CCO Ltd diving management study #5, except in Brazilian
waters, where the authorities may impose their unsuitable
modifications.
Therefore, while the adoption of the initial saturation procedures by the
Brazilian authorities in 2011 could be seen as an example to follow by
national bodies, the modifications they implemented since 2016 and
the lack of reactivity they demonstrate to correct issues should be
regarded as an example not to follow, which opens to discussion
regarding the duties of states regarding the publication and
implementation of standards.
For an accurate discussion, it is essential to remember that in an "ideal
world," governments are expected to establish standards based on
scientific research, which they either fund or adopt, in line with their
role as judges and arbitrators, ensuring that the procedures applied
within their territory adequately protect all citizens. These standards
are then adopted by companies and professional organizations, which
use them to develop their guidelines, and can be shared with other
national and international organizations.
Most governments are also engaged in the application of the World
Medical Association’s “Declaration of Helsinki on Ethical Principles for
Medical Research Involving Human Subjects”. This declaration, first
published in 1964 to prevent unethical medical practices and amended
in 1975, 1983, 1989, 1996, 2000, 2008, 2013, and 2024, is composed
of 37 articles classified into topics, among which the following refer to
procedures to implement when undertaking new studies involving
human participants:
•
Article 12, in the section “General Principle”, states that medical
research involving human participants must be conducted only by
individuals with the appropriate ethics and scientific education,
training, and qualifications, in addition to the fact that such research
requires the supervision of a competent and appropriately qualified
physician or other researcher. It also states that scientific integrity
is essential in medical research involving human participants and
that involved individuals, teams, and organizations must never
engage in research misconduct.
•
Article 17 in the section “Risks, Burdens, and Benefits” says that all
medical research involving human participants must be preceded
by careful assessment of predictable risks and burdens to the
individuals and groups involved in the study in comparison with
foreseeable benefits to them and other individuals or groups
affected by the condition under investigation. Also, measures to
minimise the risks must be implemented, and the risks and
burdens must be continuously monitored, assessed, and
documented by the researcher.
•
Article 18, also in the section above, states that physicians and other
researchers may not engage in research involving human
participants unless they are confident that the risks and burdens
have been adequately assessed and can be satisfactorily managed.
In addition, when the risks and burdens outweigh the potential
benefits or there is conclusive proof of definitive outcomes,
physicians and other researchers must assess whether to continue,
modify, or immediately stop the research.
•
Article 21 in the section “Scientific Requirements and Research
Protocols” mentions that medical research involving human
participants must have a scientifically sound and rigorous design
and execution that is likely to produce reliable, valid, and valuable
knowledge and avoid research waste. It also states that research
must conform to generally accepted scientific principles and be
based on a thorough knowledge of the scientific literature and other
relevant sources of information.
•
Article 22, which follows Article 21 in the abovementioned section,
states that the design and performance of each research study
involving human participants must be clearly described and
justified in a research protocol. This protocol should include a
statement of the ethical considerations involved and indicate how the
principles in the Declaration have been addressed. Additionally, it
should provide information regarding aims, methods, anticipated
benefits, potential risks and burdens, qualifications of the
researcher, sources of funding, any potential conflicts of interest,
provisions to protect privacy and confidentiality, incentives for
participants, provisions for treating and/or compensating
participants who are harmed as a result of participation, and any
other relevant aspects of the research.
•
Article 23 in the section “Research Ethics Committees” mentions
that the protocol must be sent for review, comments, guidance, and
approval to a relevant research ethics committee before starting the
research. That this committee operates transparently and maintains
independence from outside influences, in addition to having enough
resources. Its members must be well-educated, trained, qualified,
and diverse to assess the research effectively, suggest changes,
and eventually withdraw approval and suspend ongoing studies.
Finally, this article concludes that no protocol changes can occur
without committee approval.
•
Article 26 in the section “Free and Informed Consent” states that
each potential participant must be adequately informed in plain
language of the aims, methods, anticipated benefits, possible risks
and burdens, qualifications of the researcher, sources of funding,
potential conflicts of interest, provisions to protect privacy and
confidentiality, incentives for participants, provisions for treating
and/or compensating participants harmed as a consequence of
participation, and any other relevant aspects of the research. The
potential participant must be informed of the right to refuse to
participate in the research or withdraw consent to participate
without reprisal. Special attention should be given to the specific
information and communication needs of individual potential
participants and the methods used to deliver the information.
These articles are reused by competent international bodies such as
the “Council for International Organizations of Medical Sciences
(CIOMS)” and UNESCO and are reproduced in the Brazilian Ministry of
Health's "Operational Manual for Research Ethics Committees (Manual
Operacional para Comitês de Ética em Pesquisa)". So they should be
applied in Brazil when research is undertaken to issue a new
decompression procedure.
Given the absence of any documentation substantiating the
implementation of these articles, it can be deduced that they have
likely not been applied for the study of these Normam-222/DPC
saturation decompression procedures and the previous 2016 and
2021 revisions. This is likely due to a lack of awareness among the
individuals who imposed these US Navy procedures and probably
believed their actions were optimal.
It is worth noting that, although the Brazilian government is highlighted
here, we must recall that it is not the sole entity to publish documents
with inconsistencies made by civil servants who lack sufficient
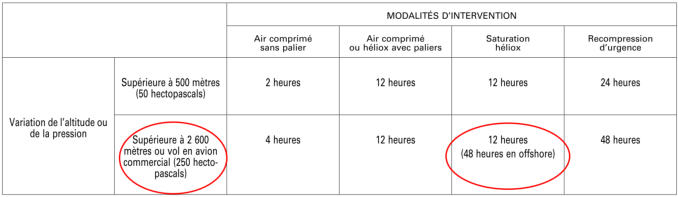
knowledge to fully understand what they write. For example, we can
note that in Section 9 of Chapter 3, “Procedures et Moyens de
Decompression”, of the “Arrete du 14 mai 2019 relatif aux travaux
hyperbares effectues en milieu subaquatique—mention A (Decree of
May 14, 2019, relating to hyperbaric work carried out
underwater—reference A)”, it is stated that a diver who has been
involved in an inshore or inland saturation dive should wait 12 hours
before being authorized to be transferred by plane with the cabin
pressure at 250 hectopascals (long-range flight), but that if this diver
had undertaken the same saturation with the same work offshore, the
standby time before flying the same distance becomes 48 hours.
Therefore, it appears that the individuals who wrote this document did
not understand that the standby time before flying is related to
decompression.
Other inconsistencies can be noted in this document.
This means that governments should employ experienced specialists
to compile and publish their directives, which must be based on
consistent reasoning and scientific evidence.
Due to the specific aspects of diving and ROV operations, some issues,
such as those related to decompression, may fall outside the
competencies of their employees. For this reason, it is common for
competently managed national organizations to appoint independent
bodies to compensate for this lack of expertise. For example, from the
1960s to the late 1990s, the French government commissioned COMEX
to develop its mandatory diving tables and related standards and
conduct research on diving physiology, which culminated in the Hydra
10 dive (reaching 701 meters) in 1992 (As mentioned above, it is
unfortunately no longer the case). It has also been the case in the
United Kingdom, where the Health and Safety Executive (HSE)
appointed organizations such as "Unimed Scientific Limited" to
undertake physiological research and provide documented guidelines
on diving procedures. It is still the case with the Norwegian
government that appoints the "Norwegian Underwater Institute" (NUI)
for similar tasks, or the Polish government that interacts with the
"Polish Hyperbaric Medicine and Technology Society", or the United
States administrations, such as OSHA (Occupational Safety and Health
Administration) and NOAA (National Oceanic and Atmospheric
Administration), that refer to the diving procedures published by the
US Navy.
These appointed organizations are distinguished by their ability to
provide documentation that adequately describes and supports the
standards they have issued, and to give the names of their authors.
This is, for example, the case of Dr. Valerie Flook, who is known to have
signed numerous UK-HSE documents and, more recently, those
published by NUI, the Polish Hyperbaric Medicine and Technology
Society, or the US Navy (see in our database).
Contrary to these examples, we are witnessing a phenomenon where
some states create mandatory standards solely based on guidelines
from various professional organizations they adopt without prior study
or consultation with competent experts, often relying only on unverified
assumptions. It is true that, due to their small size and limited budgets,
some of these states lack adequate resources and expertise regarding
underwater operations. However, nothing prevents them from
occasionally engaging advisors who could assist in selecting existing
standards and guidelines suitable for the norms they aim to establish.
We are therefore faced with a scenario opposite to the ideal, which
raises questions about the validity of the standards these states
create, adopt, publish, and approve.
Let's be clear: The problem does not lie with the professional
organizations that publish guidelines to defend their viewpoints and
achieve a certain harmony regarding the procedures applied by their
members, as they are entirely within their role by doing so. The issue
stems from the inability of some states to make appropriate decisions
for ensuring the reliability of the information they provide, which
typically falls under their responsibilities, due to the problems
mentioned above.
This often leads to illogical national standards that may then be taken
as references, encouraging the spread of other inadequate
procedures whose authors cannot justify the reasons behind them. As
these improperly founded norms accumulate erratically, they can also
become circular references, leading to a monoculture that lacks
adequate questioning of the validity of the promoted procedures. This
creates a chaotic situation where national bodies, which should serve
as references, lose their prerogatives to pressure groups, as
previously explained in the article "About Standards," published in this
section of the website in January 2023.
It is worth noting that this lack of scientific and technical supporting
documents is not only a fact of only these governments, as we can
also highlight that some well-known supranational organizations, such
as the International Maritime Organization (IMO), the International
Organization for Standardization (ISO), the European Standards, and
others commonly referenced, are known to issue standards for which
we cannot see the scientific and technical studies used or who
compiled them (except for ISO regarding this last point), which
contrasts with the virtuous behaviour we advocate, and some
organizations and states mentioned above have demonstrated that it
can be implemented.
Such a chaotic situation should not continue, or the foundation on which
safety procedures rely will vanish, potentially leading to accidents due
to a loss of fundamental knowledge and people applying rules without
understanding their basis.
Therefore, we advocate for national, supranational, and international
organizations to be exemplary in how they present their standards,
which should be thoroughly documented and validated by the scientific
and professional communities. Remember that scientific references
are now easily accessible, as many free databases are available to the
public, making it easy to provide them.
Of course, implementing such practices may be challenging for some
personnel who have worked for some time in organizations
accustomed to imposing rules without explanation or discussion. It is
therefore the responsibility of the hyperbaric workers' community to
strongly request that the standards imposed on them are based on
recognized scientific studies, cited in published documents, and
endorsed by competent scientists and the communities involved with
these norms. In other words, we can agree that those who issue
national and international standards should enforce them only if they
can explain the reasons for the norm they want to publish, on what
these new norms will be beneficial for the community, on which
scientific studies these norms are based, whether these studies have
achieved consensus regarding their conclusions, and whether the
norm will not conflict with existing ones. Additionally, the names of the
people involved in the elaboration of standards should be mentioned, as
is customary in the scientific community. Therefore, if these elements
are not adequately provided, the new standard should not be
implemented.
The second point is that this evaluation revealed that while most parts
of the saturation procedures remain unchanged, and some
improvements, such as the respect of the biological cycle of the divers,
have been provided, the Brazilian authorities made the following
modifications, resulting in these procedures no longer being compliant
with the original ones published in 2011:
•
The initial PPO2 values during the decompression phase, initially
between 0.48 and 0.5 bar, have been reduced to 0.44 and 0.48 ATA.
These absolute atmosphere (ATA) values are those used by the US
Navy revision 7 (published in 2016) for the storage and ascent
phases. Taking into consideration that a scientist would have used
pascals or, alternatively, millibars, given that the table is written in
metric units, we have concluded that this modification has not been
performed by a scientist or a diving specialist accustomed to
decompression procedures. Additionally, recent procedures
designed by Jean Pierre Imbert for reputed companies that are
IMCA members show that the value of 480-500 mb has been
maintained with equivalent storage PPO2 values to those he initially
provided for the NORMAM-15/DPC-2011. Furthermore, studies such
as the paper "Evaluation of North Sea saturation procedures
through divers monitoring" show that these tables yield very
satisfactory results regarding oxygen and decompression stresses.
Therefore, the question can be raised about the safety
performances that can be expected from new decompression
procedures that continue to use the former rates of ascent but with
lower chamber PO2.
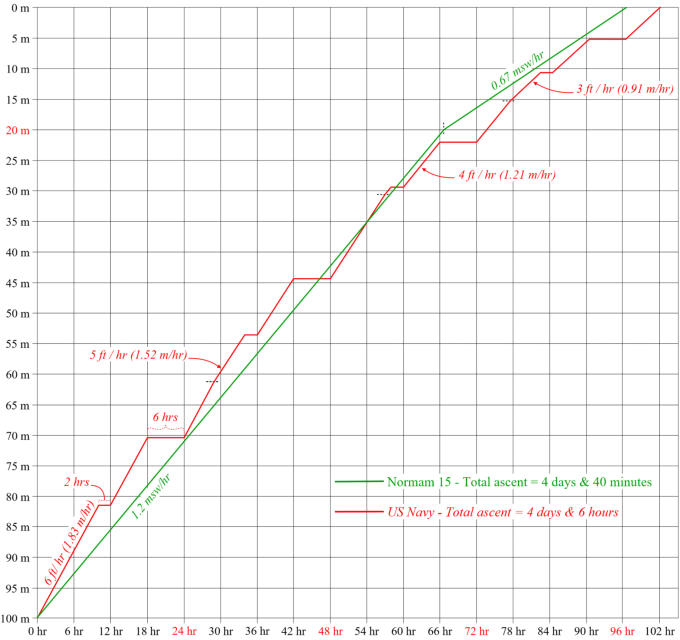
To further explain this point, it must be taken into account that the
decompression strategies of COMEX-based tables and US Navy
tables are not the same: While COMEX-based procedures such as
the Normam-15/DPC-2011 use slow, continuous, and uninterrupted
ascent rates (1.2 msw/hr from 350 to 20 m and 0.67 msw/hr from
20 m to the surface) with a PPO2 of 480 to 500 mbar after an at-
depth rest period in the living chamber (commonly called "storage")
with a PPO2 of 380 to 450 mbar, the US Navy procedures use
faster ascent rates interrupted by 8 hours of stops per 24 hours
divided into at least two parts, with a PPO2 between 0.44 and 0.48
ATA (445.83 mb - 486.36 mb) and the same PPO2 during the
"storage" period. We can note that these standby times (stops)
during the ascent compensate for the faster ascent rates
compared to the COMEX procedures (see the comparison of both
decompression curves below).
Therefore, taking into account that the decompression strategies are
different, we can consider that changing the PPO2 of the NORMAM-
15/DPC by adopting those of the US Navy resulted in creating a new
decompression procedure that should have been rigorously tested.
As a conclusion, it seems to us that no modification of these original
gas values was necessary and that this modification has been
imposed without the support of any published scientific study and
without consulting the lead author of the original procedure or
members of the scientific community, which the Brazilian
authorities implicitly confirmed in a message received on 07 August
2025, as they did not provide any documented answers to our
questions regarding this critical point.
•
The percentage of O2 during the final phase of decompression is
now limited to 21% instead of the initial 25%. While the 25% limit may
increase the risk of fire if an imprudent operator exceeds it, it
offers a comfortable operating range for the Life Support
Technicians (LST), which is significantly reduced with a limit to only
21%. Considering that the LST on duty will require a certain degree
of flexibility, we made the remark that the 23% value recommended
by IMCA, previously retained in the initial edition of the CCO Ltd
study #5, is balanced and appropriate. The Brazilian authorities
responded that the final part of the text was incorrectly edited and
should have stated that the ideal oxygen percentage must remain
within the range of 19% to 23%, with 21% as the recommended
value. Therefore, a correction is to be made to this already 9-year-
old text.
•
Note that the PPO2 values for the compression and storage phases
that were lost in the initial official 2011 document, despite being
provided by the author in the initial COMEX procedure, are still
missing in the NORMAM-222/DPC revision. The Brazilian authorities
did not comment on our remark regarding this point.
•
The excursion combination #7 “Exceptional upward excursion
followed by a standard upward excursion” has disappeared in the
document NORMAM-222/DPC. The Brazilian authorities said that it
was due to an editorial oversight at the time of publication, which
had not been formally identified until now.
Courtesy of Fabrice Pipault
Christian CADIEUX & Doctor Jean Yves MASSIMELLI