










Evolution and Performance of The Comex Tables
Author: Jean Pierre Imbert
Note:
This document was first printed in the Divers Alert Network (DAN)
recompression chamber network newsletter in February 2023.
As a reminder, DAN is an organization committed to the health and
well-being of divers, with research, medical services, and global-
response programs that create an extensive network that supports
divers with vital services such as injury prevention, safety and
educational programs, and lifesaving evacuations.
Introduction
France has a long tradition in diving, and as a consequence, in
treating bent divers.
The first account of recompression treatments was published in
1854 by Pol and Wattelle who reported 16 cases of caisson workers
experiencing CS.
Pol and Wattelle worked in coal mining in the north of France. Pol
was the engineer and Wattelle, his friend, a medical doctor. Pol ran
pressurized work to around 3 atm to prevent water ingress in the
mine shafts and of course witnessed many cases of DCS. Dr.
Wattelle described how he and Pol tried to understand the causes
and attempted to cure the unfortunate workers. They finally used
recompression to ease the symptoms. Pol was involved in the
treatment of his workers and eventually died from consequences
of severe decompression sickness after he had attended several
recompressions with his workers. In the paper, written 10 years
later, Dr. Wattelle recalled the dedication of Pol and concluded by
the sentence: “you only pay when you leave”.
In 1878, Paul Bert published his famous book, “La Pression
Barométrique”, where he demonstrated with dog experiments the
benefit of oxygen in reducing bubbles produced by a
decompression.
By the turn of last century, the development of caisson works
permitted the edition of early treatment protocols.
However, it was not until 1933 that Dr. Benkhe structured and
edited the first US Navy treatment tables. In 1965, Dr. Workmann
conducted the necessary revision work to give the treatment pro-
tocols their final form. Meanwhile, Dr. Val Hempleman designed
the Royal Navy Treatment Procedures.
The US Navy treatment tables, and in particular the Table 6, have
since remained the most used protocols, and the development of
commercial diving has permitted the publication of alternative
procedures.
At the time, Dr. Xavier Fructus was the medical advisor of Comex,
a leading commercial diving company located in Marseille. He spent
many nights on the phone, assisting work sites involved in divers’
treatment because at the time, the DCS incidence rate was around
10-15%. Based on his operational experience, Dr. Fructus developed
in 1974 the first version of the Comex Medical book, which
significantly differed from the Navy’s practice. It was designed for
a diving supervisor or a caisson master, lost on rig on the other
side of the world with a small chamber, a few gas quads, and a
fellow diver to treat, trying to establish a phone communication with
Marseille.
The 1974 Comex Medical Book
The early 70’s offered the diving companies the North Sea market
for which they were not really prepared. This was an exciting period
for the development of diving procedures, but also a time where a
lot of divers suffered decompression sickness.
Facing this situation, the medical doctors in charge started
challenging the idea that prevailed at the time: first recompress the
patient to the depth of relief. This concept was behind some deep
British treatment tables and has remained underlying the US Navy
table 6A, 1A, and 4 with their recompression on air to 50 msw (165
fsw.) However, it was known that in many cases, after the
symptoms were relieved, the patient would be too deep, and his
return to surface became a second problem.
The alternative was to restrict the recompression depth and wait
until the symptoms gradually resolved.
In 1974, Dr. Fructus edited the Comex Medical Book as a blend of
the US Navy and French Navy tables. He introduced the
revolutionary Table Cx30 that included a 30 msw maximum
recompression. His idea was to avoid deeper recompression, which
he formulated as “give time to time”.
For surface supplied operations, this first Comex medical book
included a long series of treatment tables ranging from 12 msw to
30 msw:
•
The Cx12 table, with two hours oxygen breathing at 12 msw, was
the starting point of all the treatments for pain-only
symptoms.
•
The Cx18C, with 40 minutes oxygen breathing and the Cx18 L,
with 60 minutes oxygen breathing at 18 msw (a short and
standard version of the USN Table 6) was designed as a fallback
for the Cx12.
•
The Cx30 table, which included 40 minutes at 30 msw on 50/50
gas, was the ultimate table for the recompression of severe DCS
cases.
The Cx30 was derived from a 30 msw recompression table initially
designed by Prof. Bathélémy at the French Navy Diving Department.
In the 1974 edition of the Comex medical book, the Cx30 existed in
several versions, Cx30, Cx30 A, and Cx30 AL (60 minutes on mix, or
90 minutes on air after an oxygen convulsion). The instructions
associated with the Cx30 tables only specified the oxygen
percentage without indicating the nature of the treatment mix. Dr.
Fructus kept the option for operational flexibility so that people on
board could use whatever 50/50 nitrox or heliox they had available.
However, he admitted that he already suspected that heliox was
particularly efficient in the treatment of air DCS.
The 1986 Comex Medical Book
In the 80’s, operations changed in the North Sea from platform
installation, which requires bottom work performed in saturation, to
inspection and maintenance jobs, which mostly concern shallow
structures and air diving. Dr. Philip James joined the Comex
company when air diving suddenly increased and recruited many
severe neurological DCS cases.
Dr. James was on the front line and directed a lot of Cx30 tables,
which he systematically performed using 50/50 heliox.
In 1986, there was a drastic revision of all the Comex diving
manuals, associated to the introduction of new air tables, new
saturation procedures, and of course, a revised set of treatment
tables.
Dr. Philip James was instrumental in this revision and wanted to
simplify the Comex treatment procedures. He first reduced the DCS
type identification table to only two options, simple and serious, as
for Type I/Type II in the US Navy manual.
Then, Dr. James reduced the number of treatment tables by
combining the Cx18C and Cx18L tables into a new Cx1886 table
similar to an extended USN Table 6 with 90 minutes oxygen
breathing at 18 msw. This way, three tables only could cover DCS
occurrence after surface-supplied diving.


Click on the
octopus to return to
the top of the page

The first comex medical book
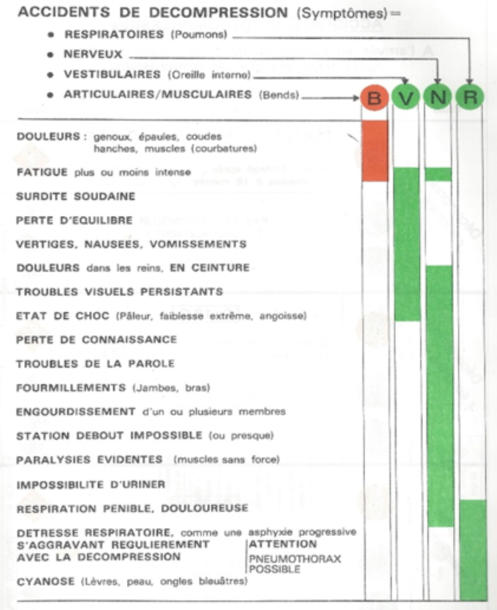
The Comex 1974 Medical Book and
its table for identification of DCS
The second comex medical book
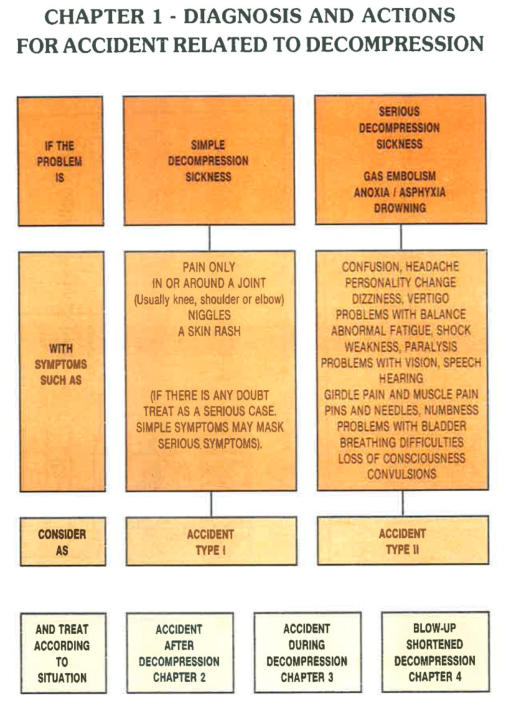
Comex 1986 Medical Book: Table for DCS Type
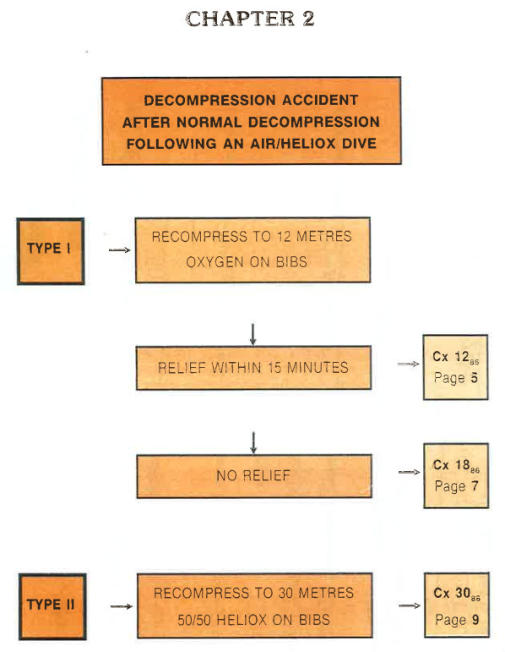
Comex 1986 Medical Book: Treatment chart
for symptoms after surface-supplied diving
Finally, Dr. James relooked the Cx30 table and gave it the format
that it has kept since. 50/50 heliox was specified, regardless of the
diving mix.
The problem with heliox was associated to isobaric counter
diffusion. The effects are sometimes beneficial, sometimes
detrimental, and they depend on:
•
The counter diffusing gases, in this case nitrogen and helium.
•
The direction of the exchanges. If the two gases changed sides,
the end result may change from super-saturation to under-
saturation.
•
The ambient pressure and thus the depth.
In Russia, at the time, Dr. Sokolov had developed a systematic
approach for the treatment of severe cases of DCS using heliox
saturation.
In Denmark, Dr. Hyldegaard conducted a series of animal
experiments and demonstrated the capacity of helium breathing to
reduce the size of nitrogen bubbles. He explained that the diffusion
of helium into the bubble combined with the diffusion of nitrogen out
of the bubble creates a situation of counter-diffusion. The result is
the shrinking of the bubble when the tissue is fatty, as can be
assumed for a neurological tissue (Hyldegaard O, Madsen J.
Influence of heliox, oxygen and N2O-O2 breathing on N2 bubbles in
adipose tissue. Undersea Biomed. Research (1989) 16: 185-193.).
He concluded the higher efficiency of 50/50 heliox breathing in the
treatment of severe DCS after an air dive. The principle was later
endorsed by DMAC (DMAC. Note 23. The Use of Heliox in Treating
Decompression Illness. 1993 – now replaced by DMAC C 23
Rev.1 – 2014).
Secondly, Dr. James modified the breathing protocol of the attendant
after one case of DCS had been recorded. In the new 1986 version,
the attendant started taking oxygen at the 12 msw stop and kept it
during the ascent to surface.
This version of the Cx30 table later became a standard in the
offshore industry through Comex and its further avatars (Stolt,
Nilson, Acergy, Subsea 7, etc.). The Cx30 was also adopted by Dr.
Yehuda Melamed for the Israeli Navy and soon appeared in many
other navy manuals (for instance, the Norwegian Navy). It finally
reached recreational diving, and DAN centers refer to the Cx30 in
several places around the world (for instance Malta Mater Dei
hospital on Malta). The Cx30 became a classic.
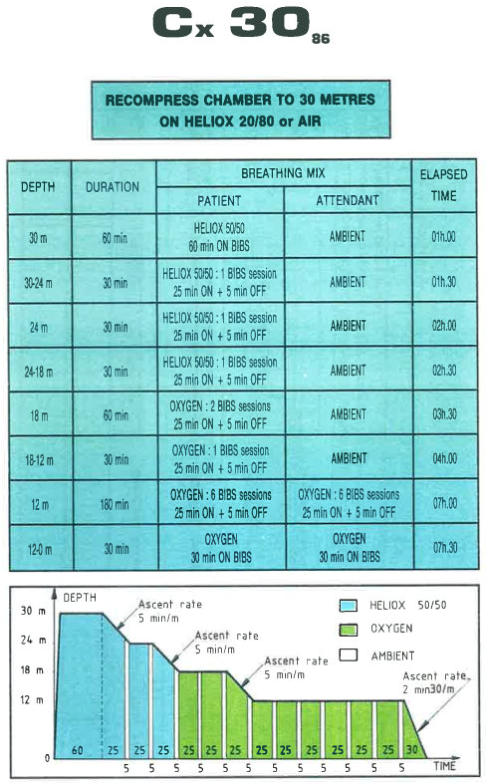
The 1986 “Classic” Comex Cx30 Table
Offshore performances of the Comex 1986 treatment tables were
published using the Comex database containing at the time around
500 treatments of DCS (Imbert, JP. Evolution and offshore
performances of the Comex Treatment Tables. Workshop on
Decompression Illness Treatment; 18-19 June 1995; Palm Beach,
Florida: Undersea Biomedical Hyperbaric Society; 1995).
The 1990 Comex Medical Book
In the 90’s, the offshore diving industry became a mature industry,
and better controlled its operating procedures.
DCS became limited to predictable cases: articular pain in the last 10
msw of saturation decompression or neurological symptoms after a
surface decompression.
In 1990, there was a new revision of the Comex diving manual and
its medical procedures.
Dr. Philip James, still in charge of the North Sea, but also Dr. JY
Massimelli in Marseille, further reduce the number of treatment
tables by eliminating the Cx18 (tables Cx12 and Cx30 were kept
unchanged).
The rationale was that if the symptoms were pain only, a Cx12
would do the job. If the symptoms were serious, compressing to 18
msw would be a waste of time since a Cx30 would be much more
efficient. It was also explained that a compression at 18 msw
provides too high a PO2 that should be optimized to around 2 bar,
which is the case in the tables Cx12 and Cx30. The decision flow
chart after a surface-supplied dive only considered two treatment
tables.
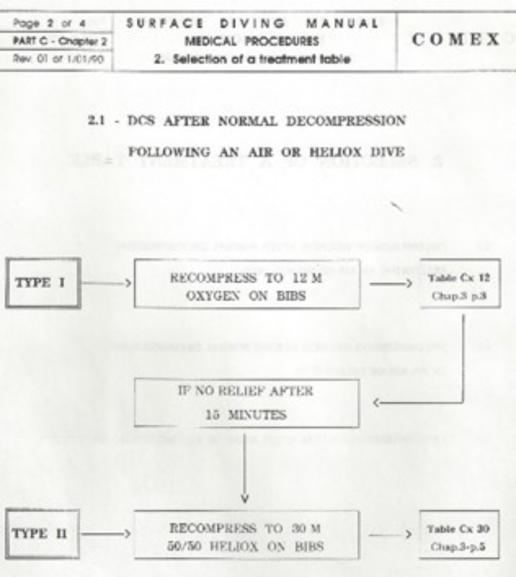
Comex 1994 Medical Treatment Chart for
Symptoms after Surface-Supplied Diving
Current Commercial Diving Practice
Today, Comex has disappeared into the history files, but its
contributions still remain. The industry has further improved and
DCS has become a rare event. Companies operating in the North
Sea report around one case of DCS every 10 years. The culture has
changed too, and the emergency medical coverage is ubcontracted
to external companies. Therefore, the trend is towards
standardization and simplification because the hyperbaric doctor in
charge will have to deal with many clients and varied treatment
procedures.
A typical decision flow chart is presented below. There is no need
anymore to make a diagnostic. The recompression starts with a
systematic Table 6 and is oriented for the rest of the treatment,
depending on the response of the patient at 18 msw. The Cx30 is
only there for the serious cases, but most of the time, the patient
benefits from successive extensions to the Table 6.
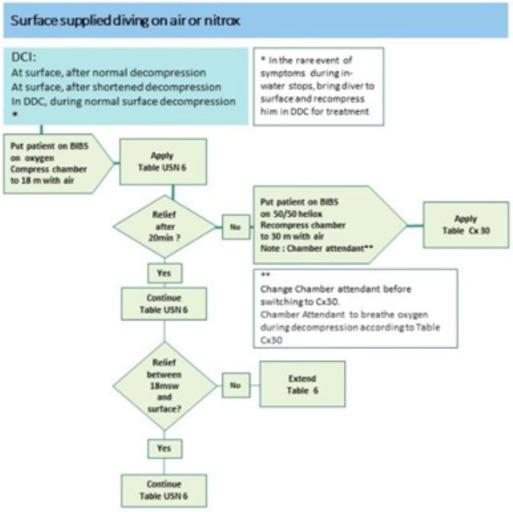
A typical offshore commercial diving medical
book in 2022
Conclusion
The Comex medical book was typical of a commercial diving
company. It came after the Navies had published their treatment
procedures and used a different experience. The treatments and
the tables were not the same.
They were also unique in a sense that Comex was very involved in
hyperbaric research. In particular, the table Cx30 has been very
successful and deep recompression treatment tables have
progressively disappeared from the diving manuals.
These original procedures also evolved with time and adapted to the
concerns raised by specific worksites. If initially the treatment
procedures were a matter of company culture, the international
dimension of the offshore industry now requires standardization,
and as a consequence, simplification.
The Comex Cx30 tables have survived this evolution and have
become an international standard, mainly prescribed as a fallback
to the Table 6 for severe cases. It still appears in many large
commercial diving manuals.
About the author:
Jean-Pierre Imbert started his exceptional career in 1975 with a
master's degree in biomedical engineering, obtained at the Institute
for Environmental Medicine in Philadelphia where he studied
isobaric counter diffusion under the direction of Dr Christian J.
Lambertsen.
From 1975 to 1995, he was part of the Comex research &
development team which led all the deep dives programs including
the CORAZ animal experimental program to 1000 msw, the manned
experimental and operational deep dives, i.e., JANUS IV 450 msw,
DRET 450 msw, JASON experimental argon saturation, and the
Hydra program using the hydrogen-helium-oxygen breathing
mixture that culminated in two world records: Hydra 8, at sea, and
Hydra 10 onshore, with 534 msw and 701 msw depth, respectively.
Being the Comex Diving Manager from 1982 to 1995, Jean-Pierre
Imbert designed the Comex diving procedures, particularly the
1986 and 1994 revisions of the Comex diving manuals and safety
management system. He designed the French government MT92
diving tables which have become an international reference, and the
deep diving operations procedures that have been published by the
Brazilian authorities as NORMAM-15/DPC. Jean-Pierre Imbert had
major participation in the Norwegian Deepex I 300 msw and II 450
msw projects at the Norwegian Underwater Institute, in the 350
msw offshore pipeline repair, and the 350 msw NorskHydro
Oseberg project.
He also designed procedures for major tunnelling interventions
accomplished in Barcelona, Hong Kong, and Singapore, and is the
author of diving manuals for diving companies.
Jean-Pierre Imbert keeps leading research & development
programs and publishing landmark scientific papers.
